BPPV is the most common inner ear cause of vertigo. It’s the classic reason someone gets a sudden spinning feeling when they roll over in bed, lie down, sit up, look up, or bend over.
The spinning can feel intense and unsettling, but the word benign means it’s not dangerous or life-threatening, even though it can feel awful when it hits.
At PhysioCentral in Miranda, we’re experienced in treating BPPV. The goal is to work out whether your symptoms really are caused by BPPV, which canal is involved, and which repositioning manoeuvre actually matches that pattern.
The good news is that ~80% of people suffering from the most common form of BPPV are symptom-free following just one treatment.
What you need to know
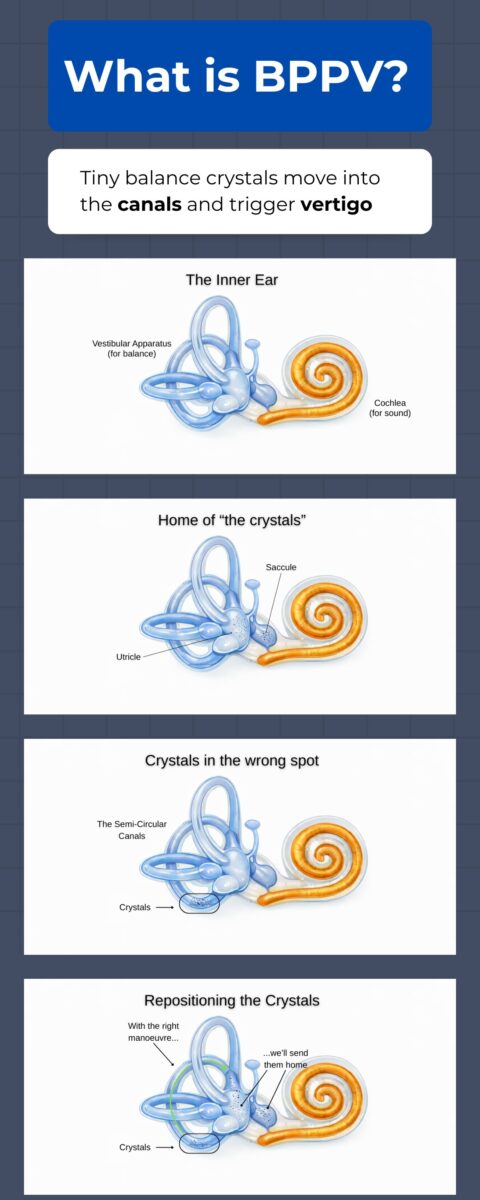
BPPV happens when tiny calcium carbonate crystals, called otoconia, become displaced from where they normally belong in the inner ear and find themselves within one of the semicircular canals.
Those crystals are sometimes referred to as “crystals”, “ear rocks”, or “ear stones.” They normally help the balance system detect movement and gravity, but once they move into the wrong place, head movement can create a false sensation of spinning.
BPPV is also more common with increasing age, and it is seen more often in women, especially around menopause. That does not mean menopause directly causes BPPV, but changes in bone health, calcium regulation, and vitamin D status may make the inner ear crystal system more vulnerable in some women.
In fact, Vitamin D deficiency has been found in about 50% of BPPV cases.
We also notice one or more of these common scenarios in people who suffer BPPV:
- they’ve recently been dehydrated
- have inconsistent water intake
- They sleep predominantly on one side
- have low blood pressure
- have recently altered certain medications
- they’ve recently been ill
- recent onset of stress or anxiety
On this page
- What BPPV actually means
- How the inner ear balance system works
- Why BPPV happens
- What causes BPPV, and who gets it most often?
- How common is BPPV?
- Common BPPV symptoms
- What BPPV usually doesn’t cause
- Canalithiasis vs cupulolithiasis
- The three canals explained
- Posterior canal BPPV
- Horizontal canal BPPV
- Geotropic vs apogeotropic horizontal BPPV
- Anterior canal BPPV
- How BPPV is diagnosed
- How BPPV is treated
- Do scans or medication help?
- Can BPPV go away on its own?
- Why BPPV comes back
- When it might not be BPPV
- BPPV treatment in Miranda
What BPPV actually means
BPPV stands for Benign Paroxysmal Positional Vertigo.
- Benign means it isn’t usually dangerous
- Paroxysmal means it comes in sudden, short spells
- Positional means it’s triggered by head position or head movement
- Vertigo means a false sense of spinning or motion
That definition matters because it clearly describes the pattern. BPPV usually causes brief, position-triggered spinning rather than constant, all-day dizziness.
How the inner ear balance system works
The inner ear has two main jobs. The cochlea handles hearing, and the vestibular apparatus handles balance and position.
The vestibular apparatus includes the semicircular canals, the utricle, and the saccule.
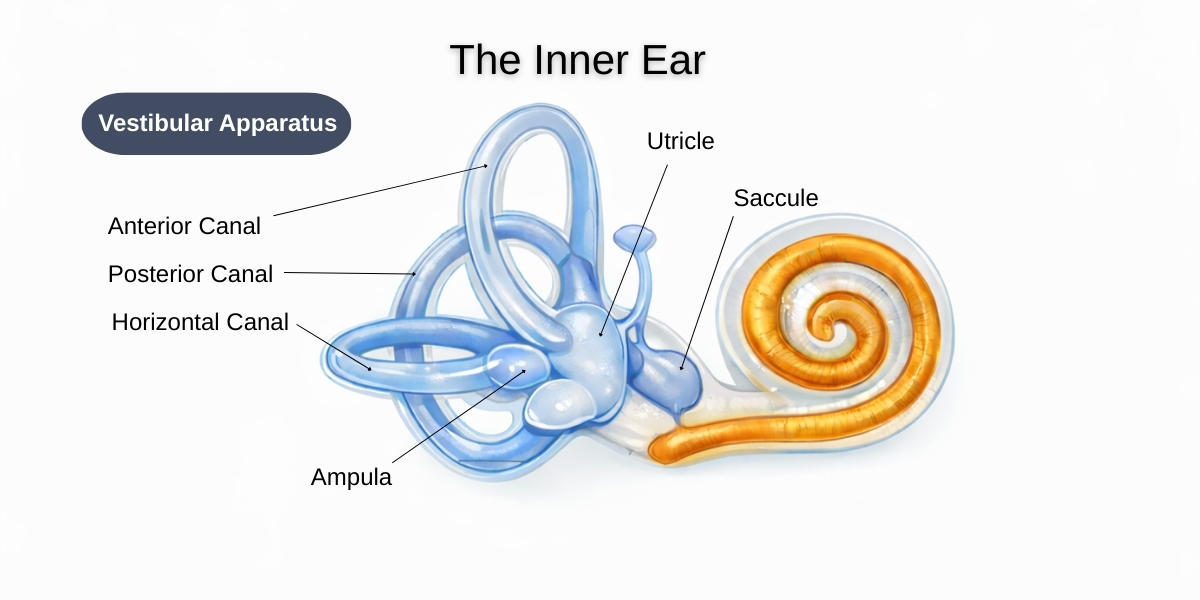
The utricle and saccule are called the otolithic organs. They help detect straight-line movement, like moving forward in a car or going up in a lift. They contain the otoconia, those tiny calcium carbonate crystals that normally sit where they belong and help the brain detect motion and gravity.
The semicircular canals are different. They detect rotational movement. There are three of them, and each one sits in a different plane to sense a different direction of movement.
- The anterior (superior) canal senses up and down movement of the head, like nodding “yes”
- The horizontal (lateral) canal senses rotating movement of the head, like shaking your head “no”
- The posterior canal senses tilting movement of the head, like bringing your ear toward your shoulder
That simple picture helps explain why different head positions trigger different BPPV patterns.
The posterior canal is the most common version. The horizontal canal is the next most common and is easy to miss if someone assumes every case is standard BPPV. The anterior canal is the rarest.
At the base of each semicircular canal is a widened area called the ampulla. Inside that area is the cupula, which is a gel-like structure linked to the hair cells.
When your head moves, the inner-ear fluid shifts and pushes on the cupula. That bends the hair cells and sends a signal to the brain that you’re turning.
In BPPV, misplaced crystals disturb that signal, so the brain gets told you’re moving more than you really are.
Why BPPV happens
BPPV starts when some otoconia become dislodged from the utricle and end up inside one or more of the semicircular canals instead.
Once that happens, a head movement that should feel normal can suddenly create a strong false motion signal. These tiny crystals fall through the canal like an avalanche triggering an extreme sensation of rotation making you feel like you’re spinning. It can at times be an overwhelming, violent sensation. During the sensation, your eyes can be seen as rapidly shaking which further amplifies the effect.
That’s why BPPV feels so dramatic, even though the underlying problem is mechanical.
This is also why BPPV is so position-specific. It isn’t just “dizziness.” It’s a movement-triggered crystal problem.
The exact symptoms depend on:
- which canal the crystals are affecting
- whether they’re free-floating or stuck
- which direction they move when your head changes position
What causes BPPV, and who gets it most often?
In many cases, BPPV starts without one clear trigger. A large share of cases are considered idiopathic, which means there isn’t a single obvious cause found. That’s one reason people are often surprised when it seems to come out of nowhere.
That said, some people are more likely to develop it than others. BPPV becomes more common with increasing age, and it’s seen more often in women than men. It’s also linked more strongly with factors such as:
- head trauma
- migraine
- inner ear disease
- vitamin D deficiency
- osteopenia
- osteoporosis
This is one reason BPPV is often seen more often in women around and after menopause. That doesn’t mean menopause directly causes BPPV, but changes in bone health, calcium regulation, and vitamin D status may make the inner ear crystal system more vulnerable in some women.
How common is BPPV?
BPPV is one of the most common causes of vertigo.
In a large population-based study, the lifetime prevalence was about 2.4% or 1 in 40.
One study of over-55s found that it affected just over 27% of people. Close enough to 1 in 3.
It also becomes much more common with age. In that same study, the 1-year prevalence in people over 60 was almost seven times higher than in adults aged 18 to 39.
That matters because in older adults, BPPV isn’t just unpleasant. It can also affect confidence in walking and daily movement, and increase the risk of falls. That’s one reason it’s worth diagnosing properly rather than just waiting and hoping it passes.
Common BPPV symptoms
The most classic BPPV story is brief spinning (typically 3 – 10 seconds) when you:
- roll over in bed
- lie down
- sit up
- look up or down
- bend over
People often describe it as a sudden room spin, a strong wave of vertigo, or a violent “whip” when they move their head a certain way.
Nausea is common, and some people feel a bit washed out or off-balance for a while after the spinning stops.
The key thing is that the spells are usually short and triggered. BPPV tends to come in bursts with certain movements rather than causing a constant all-day spin in the same way.
What BPPV usually doesn’t cause
Classic BPPV usually doesn’t cause:
- hearing loss
- fainting
- a completely constant non-stop severe vertigo with no clear positional trigger
That doesn’t mean every dizzy person has BPPV. It means BPPV has a recognisable pattern, and if the story doesn’t fit, the diagnosis needs a second look.
Canalithiasis vs cupulolithiasis
These two words matter because they help explain why one BPPV case behaves like a quick burst and another feels more stubborn.
Canalithiasis
Canalithiasis means the crystals are free-floating inside the canal.
When you move your head, they move, then settle. That usually creates the classic short, triggered spell of vertigo.
This is the most accepted explanation for most BPPV cases.
Cupulolithiasis
Cupulolithiasis means the crystals are thought to be stuck to the cupula, or at least acting like they’re affecting the cupula directly.
Because the cupula is the motion sensor, that can make the response last longer or behave differently.
In easy terms, canalithiasis is more like loose snow moving around in a tube. Cupulolithiasis is more like that snow sticking onto the sensor itself.
Why this matters
If the crystals are moving freely, the pattern is usually more straightforward. An easy fix.
If the crystals are sticking or behaving close to the sensor, the pattern can be more persistent, more confusing, and sometimes harder to clear in one go. More stubborn.
The three canals explained
Posterior canal
This is the most common BPPV canal.
It’s the classic version that often causes spinning with rolling in bed, lying back, looking up, or bending.
When most people talk about “typical BPPV,” this is what they mean.
Horizontal canal
This is also called the lateral canal.
It’s the next most common version and often causes a much stronger spinning sensation when the person rolls from one side to the other while lying down.
It can look and feel different enough that it gets missed if someone assumes every case is posterior canal BPPV.
Anterior canal
This is the rarest canal involved.
It’s real, but uncommon, and the positional eye movement pattern can be trickier to interpret.
Posterior canal BPPV
Posterior canal BPPV is the version most likely to give the classic story of brief spinning when rolling in bed, lying back, or looking up.
It’s usually tested with the Dix-Hallpike manoeuvre.
If the pattern fits, it’s often treated with a canalith repositioning manoeuvre such as the Epley or Semont style manoeuvre.
This is the form most home videos online are trying to treat.
That’s useful when the diagnosis is right, but it’s also why some people keep repeating an Epley at home and don’t get better.
Sometimes it isn’t posterior canal BPPV at all. Sometimes it’s a different canal. Sometimes the side has been guessed wrong. Sometimes the first treatment simply hasn’t fully cleared the crystals yet.
Horizontal canal BPPV
Horizontal canal BPPV often causes a very strong spinning feeling when the person rolls side to side in bed.
The test used here is usually the supine roll test, where the head is turned while lying on the back and the clinician watches the eye movement carefully.
This form is important because the eyes can beat in two different ways during testing: geotropic or apogeotropic.
Those words sound technical, but they simply describe the direction of the eye movement during the roll test.
That direction helps tell us what the crystals are probably doing and which manoeuvre is more likely to help.
Geotropic vs apogeotropic horizontal BPPV
Geotropic
In geotropic horizontal canal BPPV, the eye movement beats quickly toward the ground during the roll test.
This is the more classic horizontal canal pattern and is usually linked with canalithiasis, meaning free-floating crystals in the horizontal canal.
Apogeotropic
In apogeotropic horizontal canal BPPV, the eye movement beats quickly away from the ground during the roll test.
This is often the trickier version. It has traditionally been linked with cupulolithiasis, but the key clinical point is that it behaves differently and often needs a different repositioning approach.
Why this matters
Geotropic and apogeotropic aren’t just fancy labels.
They’re one of the main reasons an accurate assessment matters. The manoeuvre that helps one may not be the manoeuvre that helps the other.
Anterior canal BPPV
Anterior canal BPPV, also called superior canal BPPV, is rare.
It usually creates a different positional eye movement pattern from the more common forms, and it needs a careful assessment because some other causes of positional dizziness can look similar.
Because it’s rare, it’s easier to either miss it or over-call it.
In practical terms, it’s a variant that needs more clinical care than the classic posterior canal story. It can still be treated quickly, easily, and successfully. It just needs to be accurately diagnosed.
How BPPV is diagnosed
BPPV is usually diagnosed with bedside positional testing, not by routine scans.
The diagnosis depends on putting the head into specific positions that move the crystals and then watching for a characteristic eye movement, called nystagmus.
That eye movement is what tells the clinician which canal is involved and what sort of BPPV pattern is most likely present.
The two most common tests are:
- the Dix-Hallpike test, mainly for posterior canal and sometimes anterior canal patterns
- the supine roll test, which is used for horizontal canal BPPV
The key isn’t just whether the test makes you dizzy. It’s the combination of your symptoms and the exact direction and behaviour of the eye movement.
How BPPV is treated
The main treatment for BPPV is a canalith repositioning manoeuvre.
That means using a sequence of head and body positions to guide the crystals out of the wrong canal and back toward where they stop causing trouble.
It’s a bit like solving one of those ball-bearing maze puzzles, where you tilt the puzzle in all sorts of different angles to get the metal ball into place to complete the puzzle.
We do the same thing with your head. One position after another, in the correct sequence, so that when you sit up, the crystals fall into place.
The whole point is to fix the mechanical crystal problem, not just mask the symptoms.
For posterior canal BPPV, that often means an Epley or similar manoeuvre.
For horizontal canal BPPV, treatment may be very different, especially when deciding between geotropic and apogeotropic patterns.
For anterior canal BPPV, another manoeuvre may be used again.
This is why accurate canal-specific diagnosis matters so much.
More than one session isn’t unusual. A first treatment can be partly effective, the crystals may not clear completely, or the pattern may be more complex than it looked at first.
That doesn’t automatically mean the diagnosis is wrong. It often means the case needs a follow-up review and another well-targeted attempt.
And sometimes when we clear one canal, some of the crystals can fall into another canal. This is known as cross canal contamination.
Rare. Unfortunate. But easily rectified.
Do scans or medication help?
Routine imaging doesn’t confirm BPPV.
Depending on your symptoms, they can help rule out
Scans and standard lab tests don’t diagnose it, which is why positional testing is so important.
Some medications can desensitise the inner ear to help with symptoms, but they don’t put the crystals back where they belong.
In plain language, medication may sometimes ease nausea or distress for a short time, but it doesn’t fix the actual crystal problem. The repositioning manoeuvre is what fixes the issue.
Can BPPV go away on its own?
It can!
Most BPPV settles on its own in about 3 weeks. They tend to find there way back home through the affected canal via normal natural movement.
The problem is, people can be so worried about triggering their vertigo, that they slow down the speed of their movement, or completely avoid putting their head in some positions out of fear, not realising that this behaviour can perpetuate the symptoms, or stop them resolving on their own.
But waiting it out isn’t always the best choice.
For some people, especially older adults, that can increase falls risk and make day-to-day life harder than it needs to be.
Why BPPV comes back
BPPV can recur.
Some people have one episode and never get it again. Others have it settle, then return months or years later.
The good news is that recurrence doesn’t usually mean anything sinister. It usually means the crystal problem has happened again, and it can often be treated successfully again, especially when the exact canal pattern is identified properly.
Each recurrence tends to be less intense and less frequent.
When it might not be BPPV
Not every dizzy episode is BPPV.
If the symptoms are constant, not clearly position-triggered, linked with hearing loss, fainting, or a pattern that just doesn’t fit, then another diagnosis needs to be considered.
If dizziness comes with severe headache, double vision, weakness, facial droop, trouble speaking, fainting, or major difficulty walking, that needs urgent medical assessment.
Those features don’t fit a straightforward BPPV story and shouldn’t be brushed off as “just crystals.”
BPPV treatment in Miranda
If you keep getting brief spinning when you roll in bed, lie down, sit up, look up, or bend over, BPPV is one of the first things worth checking properly.
At PhysioCentral in Miranda, we assess whether the pattern really fits BPPV, work out which canal is most likely involved, and use the right treatment for the actual variant in front of us.
That matters because posterior canal BPPV is common, but it isn’t the only type. Horizontal canal BPPV can behave very differently; geotropic and apogeotropic patterns aren’t treated the same way, and anterior canal BPPV is rare but real. Some cases also involve free-floating crystals, called canalithiasis, while others are more stubborn and behave like crystals are affecting the cupula, called cupulolithiasis. When you combine canal type with crystal behaviour, BPPV becomes much more specific than most people realise, which is why proper assessment usually gets better results than trial-and-error home treatment.
The aim is simple: identify the right pattern, use the right manoeuvre, and help you quickly and safely get back to normal.
Trusted sources behind this page
- American Academy of Otolaryngology, Patient Information: Frequently Asked Questions: Benign Paroxysmal Positional Vertigo (BPPV)
Good for the plain-English overview of what BPPV is, what it feels like, and why it usually responds well to the right treatment. - American Academy of Otolaryngology, Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (BPPV)
Good for the clinical standard of care, including accurate diagnosis, avoiding unnecessary scans, and using the right repositioning manoeuvres. - NCBI Bookshelf (StatPearls), Benign Paroxysmal Positional Vertigo
- Useful for the medical background, bedside testing, and the point that many cases are idiopathic.
- von Brevern et al, Epidemiology of benign paroxysmal positional vertigo: a population based study
Best for the prevalence and incidence figures, including how common BPPV is and how much more common it becomes with age. - Jeong, Benign Paroxysmal Positional Vertigo Risk Factors Unique to Perimenopausal Women
- Useful for the careful wording around female-specific risk, menopause, hormonal changes, bone health, and calcium-related factors.
- NCBI Bookshelf (StatPearls), Orthostatic Hypotension
- Helpful for separating true BPPV from other common causes of dizziness, like standing-related blood pressure drops, dehydration, and medication effects.
- Vestibular Disorders Association, Peripheral Vestibular System – The Inner Ear
- Useful for the easy-reading anatomy explanations of the utricle, saccule, otoconia, semicircular canals, ampulla, and cupula.